Novel biomarker predicts how non-small cell lung cancer will progress after immunotherapy
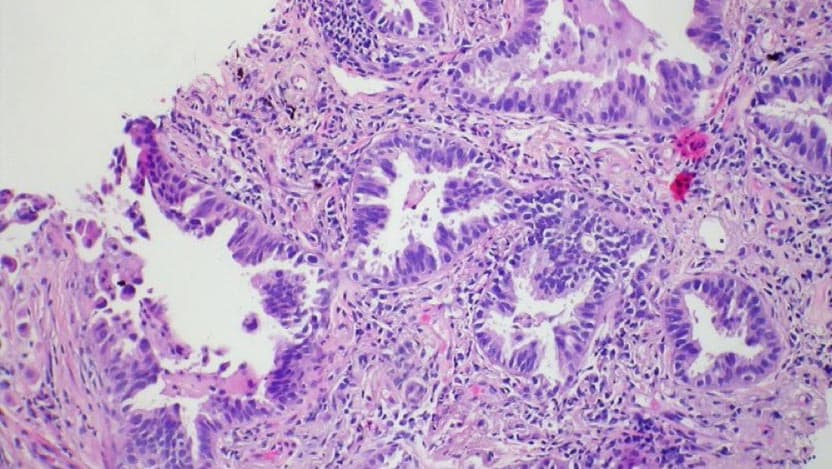
Non-small cell lung cancer (NSCLC) accounts for about 85% of all lung cancers and is the leading cause of cancer-related mortality in the U.S.
A form of treatment known as immune checkpoint blockade (ICB) improves clinical outcomes in patients diagnosed with NSCLC; however, there is limited data about what genes can predict the progression of the disease after treatment with ICB. Recently, researchers at the University of Chicago Medicine Comprehensive Cancer Center identified a novel biomarker for predicting the progression of NSCLC after ICB therapy.
“A large fraction of patients don’t benefit from immunotherapy and, therefore, it’s very important as doctors we give the right therapy to the right patient at the right time,” said Sean Pitroda, MD, Assistant Professor of Radiation and Cellular Oncology at UChicago Medicine. “Part of that is using biomarkers to identify which patients are most likely to respond to therapy.”
To this end, researchers led by Pitroda identified a tumor suppressor gene, CDKN2A, that’s loss of function was associated with inferior outcomes of ICB treatment in patients with NSCLC. These results present a novel biomarker and potential target for therapy in a large subset of patients with this disease.
A large fraction of patients don’t benefit from immunotherapy and, therefore, it’s very important as doctors we give the right therapy to the right patient at the right time.In the